
The case for value-based care (VBC) has been evident for decades, but why has it taken so long for healthcare providers to embrace it? “It’s a mindset. ‘This is what we’ve always done,’ is the excuse,” says Bill Wynn, Vice President of Strategic Partnerships, VirtuSense Technologies. “COVID-19 has been the catalyst to start shifting providers toward a mode of value-based thinking and has highlighted the need to diversify revenue streams by augmenting fee-for-service (FFS) income with VBC.”
Various legislation and programs have been approved over the past decade, but a universal implementation of value-based healthcare still alludes most care providers. The biggest barriers for initiating VBC, according to the 2019 survey by Definitive Healthcare, are lack of resources like staff shortages and integrated health IT systems; access to healthcare data; and unpredictable revenue streams—i.e. determining the financial risk involved in population health management.
“The way we’re delivering care is becoming financially prohibitive,” Wynn notes. “When looking at the months where the COVID-19 impact was biggest, providers that operated on the VBC model were still making money, but other providers that make most of their money from elective procedures and are FFS-based didn’t, because they didn’t have patients coming in.”
In September 2020, CMS issued guidance to healthcare providers to accelerate the adoption of VBC. “Many states have made progress in moving toward value-based payments in healthcare, yet there are still growth opportunities for more states to improve health outcomes and efficiency across payers including Medicare, Medicaid, and private insurance, by ensuring healthcare systems are financially incentivized to deliver the best quality, best value care. Aligning value-based care programs across payers could reduce the burden on providers who participate with multiple payers and improve the healthcare experience for patients.”
Resetting the Healthcare Trajectory
“The reason the healthcare industry is so slow in adopting a VBC model, is because providers are trained to fix things. The mindset of VBC is to never get to a point where you have to fix anything because you’re keeping your population healthy,” explains Dr. Tom Hale, Chief Medical Officer, VirtuSense Technologies. “Our current healthcare system is not preventative or patient-centric. It’s very much reactive.”
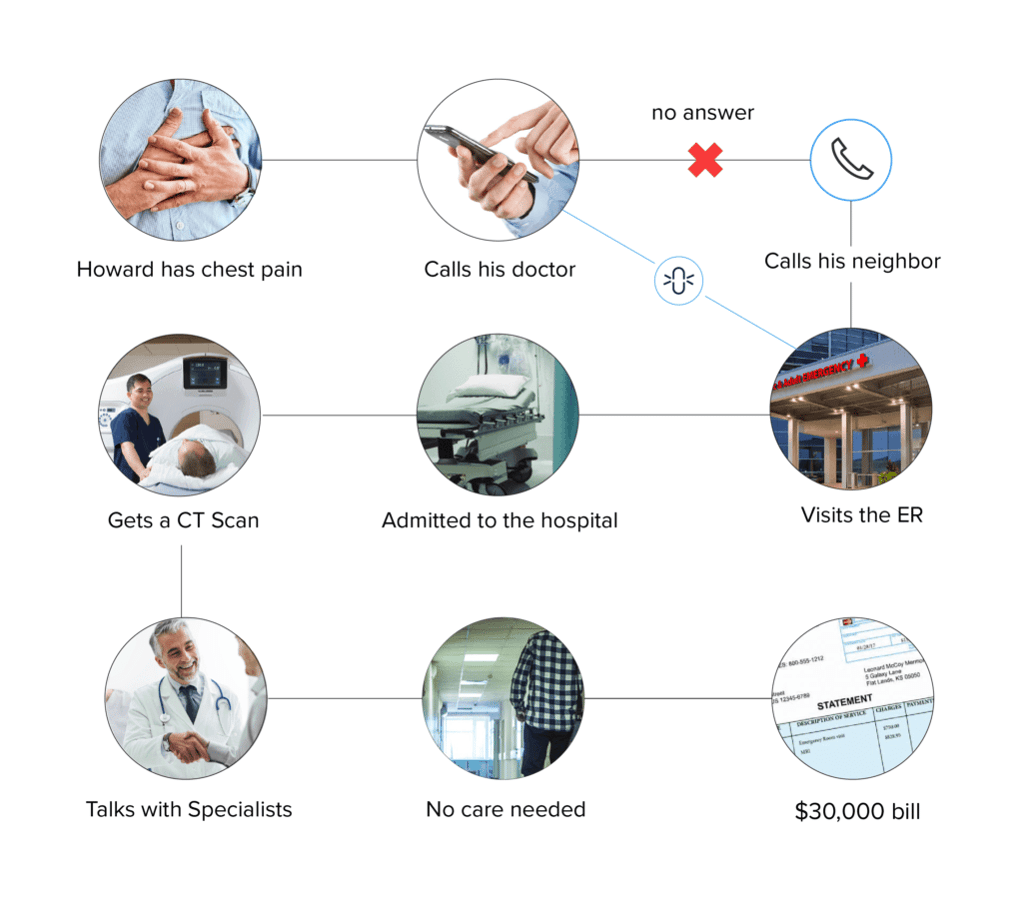
Here’s a typical scenario Hale gives to illustrate the inefficiencies of FFS. “Howard is having mild chest pain, so he calls his doctor, but the doctor either doesn’t get back to him right away or he can’t get in, so he calls his neighbor who advises him to to go to the emergency room. Howard goes to the emergency room—mind you, the ER is disconnected from the primary care physician. The ER doctor says, ‘Since you have chest pain, I’m going to admit you.’ They run a series tests, do a CT scan of the heart, and seek the advice of several specialists. At the end of the day the doctor determines Howard has chest wall pain, and that it’s not a problem. Now there’s a $30,000 medical bill, all because Howard couldn’t get timely access to his physician.”
Lack of access and increased variation contribute to an environment that encourages higher and unnecessary utilization. “We have created the perfect model and infrastructure to get the results that we are getting—i.e. a model of care delivery that is inaccessible to patients, inefficient for providers, and wasteful and expensive,” Hale notes.
“The United States spends more on healthcare than any other country, with costs approaching 18% of the gross domestic product (GDP). Prior studies estimated that approximately 30% of health care spending may be considered waste. Despite efforts to reduce over-treatment, improve care, and address overpayment, it is likely that substantial waste in US health care spending remains.” – Waste in the US HealthCare System
If You Build it They Will Come
Healthcare has built an infrastructure that creates $3 trillion in spending per year. It is an infrastructure centered around hospitals and specialists that requires a high degree of utilization in order to financially survive. “It is what I like to call ‘Feeding the Beast’ — the healthcare beast. VBC changes the dynamic. The economic driver is based on keeping people well and out of hospitals and, by necessity, can only work if there is increased access to caregivers and providers and a decrease in the variation of care delivery and a navigated pathway for the patient’s healthcare journey,” Hale explains.
“Virtual care is the engine that will drive the success of a value-based healthcare model utilizing the technologic tools, data analytics, and AI and maintenance of the relationship between the caregivers and providers. The first two are occurring rapidly in all other industries, and the third is the ‘art of medicine’ applied through a different medium.”
According to Hale, VBC needs to be a healthcare community endeavor. “Build the infrastructure around the doctors so they are able to do the right thing. The FFS economic model causes physicians to be bricklayers rather than being able to use their talents to be a general contractor. The physician/bricklayer, sees a patient and treats them, then moves on to the next one. The physician as a contractor, manages a population, which requires a more proactive approach to care.”
Hale points out that VBC thrives on access, decreased variation in care (through centralization of the data) with intelligent distribution of the knowledge and support generated by that data—a 360-degree view of a patient’s health history, versus snapshots. Access is created through a multimodal approach which includes synchronous and asynchronous communication, telehealth communication tools, and a team care approach based in patient-centricity.
Bridging the Technology Gap
“The difficulty in creating models which utilize virtual tools and data acquisition technologies is not the availability of the tools, but rather the transition in the infrastructure models. The economics have to work in the transition phase—the best of the past needs to be carried forward to the future and the pace of transformation needs to be certain that patients, providers and caregivers are not left behind,” he says. “This is evolution not revolution.”
Remote patient monitoring (RPM) technologies and telehealth options are a big part of the solution for VBC because it decreases in-person visits and hospitalizations and keeps people healthier, especially during a pandemic. It also increases access to healthcare providers so you avoid costly scenarios like the one above with Howard.
In the 2021 Physician Fee Schedule CMS is expanding its reimbursements for RPM and telemedicine and has commissioned a study of its telehealth flexibilities provided during the COVID-19 public health emergency. “The study will explore new opportunities for services where telehealth and virtual care supervision, and remote monitoring can be used to more efficiently bring care to patients and to enhance program integrity, whether they are being treated in the hospital or at home.”
“The inherent core to value based care is to keep people healthy. The tools, like remote patient monitoring, asynchronous communication, and Artificial Intelligence/Machine Learning create the ability to be the patient’s ‘general contractor’ as well as their personal physician and friend,” Hale explains. “Healthcare costs go down, profits go up, and patients have better outcomes from the proactive care that is created.
“Everybody wins.”
This article originally published here.